Subcutaneous Ureteral Bypass in a Cat
August 26, 2025 · Cats
 - Subcutaneous Ureteral Bypass in a Cat")
Signalment: 7 year old, MN Domestic
Short Hair History: Presenting to Austin Veterinary Emergency and Specialty Center Internal Medicine Department for evaluation of acute vomiting, anorexia, and concern for right-sided nephrolithiasis and ureteral obstruction.
On November 9, 2024, the patient began vomiting and became acutely anorexic. After transient improvement, clinical signs recurred on November 11, prompting evaluation with his primary care veterinarian, where radiographs revealed right kidney enlargement and a possible nephrolith.
He was referred to AVES Internal Medicine and hospitalized through the ER service. Supportive care resulted in rapid biochemical improvement, and the obstruction was presumed to have resolved spontaneously. However, at a recheck on November 21, the patient’s clinical condition declined with recurrent severe azotemia, pelvic dilation, and hyperkalemia.
Diagnostics: 11/21/24 AVES Internal Medicine - Kidney panel: Cr 13.6, BUN >130, Phos 15.1, tCa 9.4, Na 153, K 7.8
IM Urinary Ultrasound (Figure 1): Right kidney hydronephrosis (~1.3cm) with proximal ureteral dilation

Figure 1. Right renal pelvis is dilated at 1.3 cm
Diagnosis: Right, proximal ureteral obstruction
Treatment: A right-sided SUB 3.0 device was placed on November 22, followed by rapid normalization of renal values (see below)
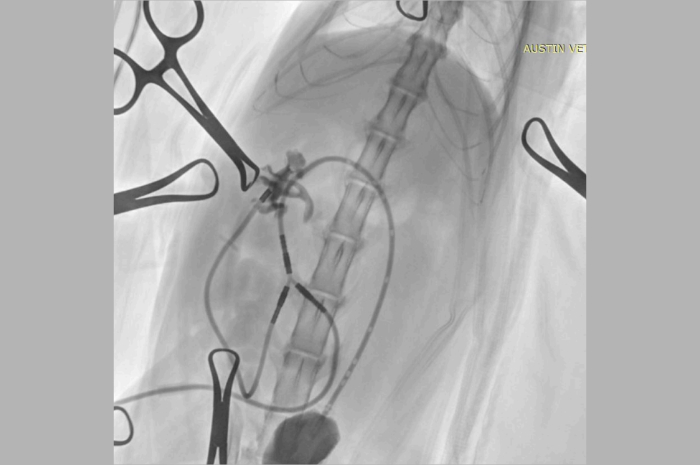
Figure 2. Fluoroscopic images of the lateral/dorsal abdomen: nephrostomy tube is within the proximal ureter and the cystostomy catheter is at the apex of the bladder. Contrast is seen in both the renal pelvis and the bladder. No leakage of contrast identified. There is a proximal ureteral obstruction on the right side. There are no kinks seen in the tubing.
11/23/24 AVES Critical Care: - Kidney panel: Creat 2.9 H, BUN 46 H, K 3.8 WNL
11/24/24 AVES Critical Care: - Kidney panel: BUN 20 mg/dL (N), Crea 1.6 mg/dL, K 3.3 mmol/L.
Outcome: Subsequent rechecks from December 2024 through April 2025 have shown stable clinical condition, successful SUB device function, and generally well-controlled renal values. SUB flushes have remained uncomplicated, and the patient has tolerated therapy well.
Ongoing monitoring is scheduled every 3–4 months with pre-visit buprenorphine recommended.