Austin Veterinary Emergency & Specialty (AVES)
Depressed Skull Fracture With Neurologic Deficits

Overview
Signalment: 7-year-old neutered male Pomeranian
Presenting Complaint: The patient was attacked by another dog and initially stabilized at an outside emergency hospital. He was transferred to AVES for continued evaluation due to persistent nonambulatory tetraparesis.
Medical History:
Vaccinations: Up to date
Travel history: None
Concurrent medical conditions: None
Medications at Presentation:
Gabapentin
Meloxicam
Clavamox
Physical Examination
Temperature: 100.9°F
Heart Rate: 100 bpm
Respiratory Rate: 34 breaths/min
Weight: 4.13 kg
A puncture wound with scab formation was present on the dorsum of the cranium, which had been shaved at the referring hospital. No other significant abnormalities were noted on physical examination.
Neurologic Examination
Mentation: Appropriate
Gait/Posture: Nonambulatory tetraparesis, more severe in the hind limbs and on the left side
Cranial Nerve Function: Normal
Postural Reactions: Absent in both left limbs; normal in both right limbs
Spinal Reflexes: Normal in all limbs
Epaxial Palpation: No discomfort noted
Nociception: Not assessed (motor function present in all limbs)
Diagnostics
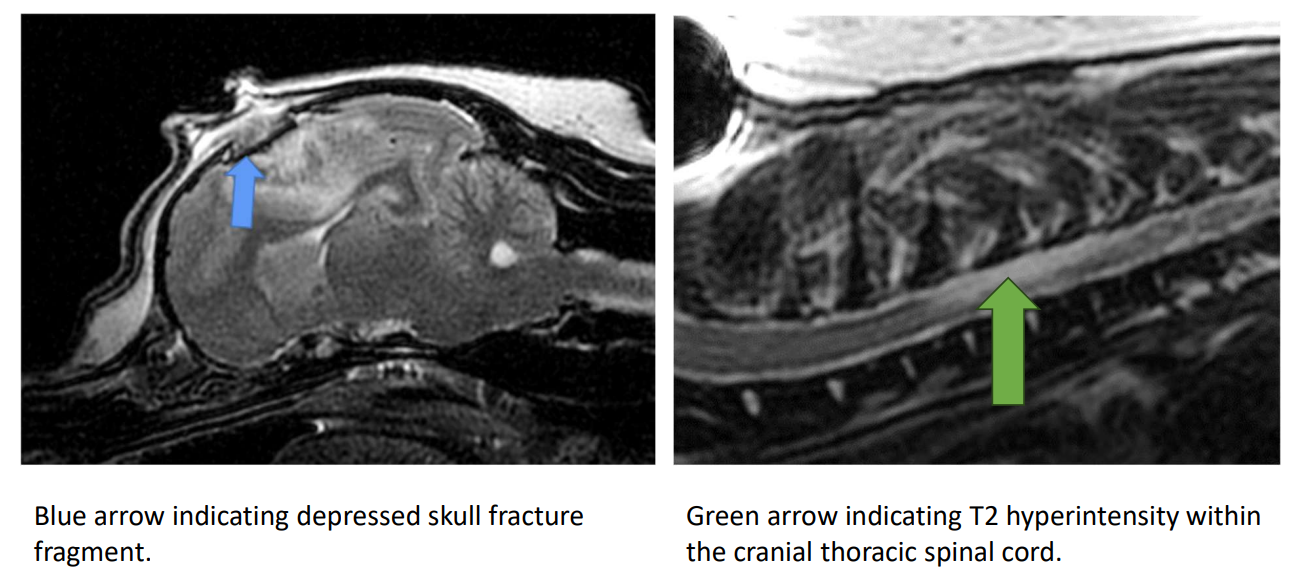
MRI (Brain and Cervical Spine):
Prominent depressed skull fracture affecting the right dorsal aspect of the cerebrum, with associated right cerebral hemorrhage and edema. Mild leftward deviation of the falx cerebri was noted.
Multifocal T2-weighted hyperintensity within the cervical and thoracic spinal cord. Differential considerations included spinal cord contusion, fibrocartilaginous embolism, and/or edema.
Treatment and Management
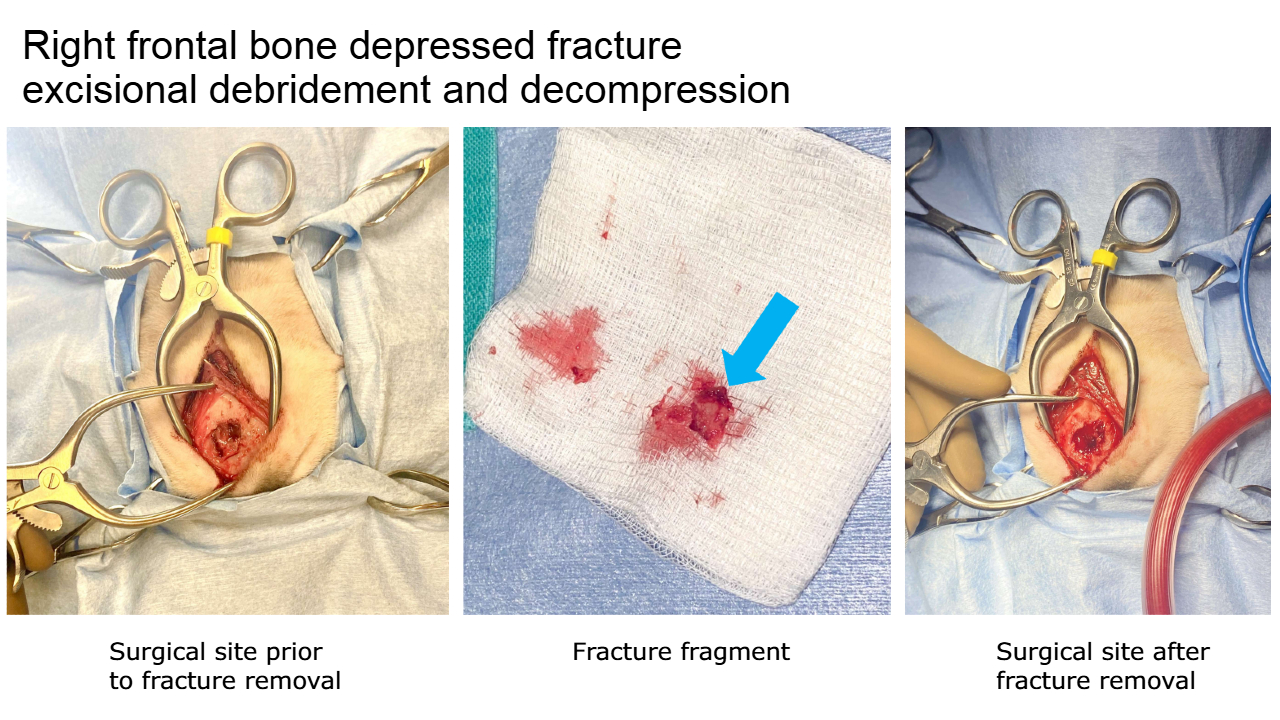
Given the depressed nature of the skull fracture, surgical decompression with excision of the fracture fragment was recommended. The potential impact of the spinal cord hyperintensities on neurologic recovery was discussed with the owner. Despite these concerns, the owner elected to proceed with surgery.
Procedure Performed: Right frontal bone depressed fracture excisional debridement and decompression.
Postoperative Progress
One day postoperatively, the patient demonstrated marked neurologic improvement. Although still requiring assistance to ambulate, he showed significantly stronger motor function in all limbs compared to his preoperative status.
Outcome
The patient was discharged on:
Enrofloxacin
Clavamox
Gabapentin
Levetiracetam
At the two-week postoperative incision check, the patient was strongly ambulatory with mild residual tetraparesis and ataxia. Additional findings included reduced menace response in the left eye and subtly decreased proprioception in the left limbs.