Blood Patch Pleurodesis
Case Study

Introduction
Pneumothorax can occur for a variety of reasons, from trauma to spontaneous bullae rupture to iatrogenic to neoplasia. In some cases, such as blunt force trauma, conservative care is appropriate. In other cases, such as neoplasia or large bullae, surgery is ideal. Even after appropriate care (whether conservative management or surgery), pneumothorax can persist. Performing a blood patch pleurodesis is a inexpensive, relatively easy and relatively minimally invasive method that can yield good results.
What is a blood patch pleurodesis?
Blood patch pleurodesis (BPP) is the process of injecting fresh whole blood (usually autologous) into the pleural space of a patient with pneumothorax using a chest tube. This process aims to mechanically seal an air leak via clot formation as well as induce a mild inflammatory pleurodesis, promoting pleural surfaces to adhere and prevent further leaks.
Why and when?
Can be considered for persistent pneumothorax that have failed surgical or conservative management.
Typically if persistent for >2-5 days after surgery, trauma, etc
Can also be considered for pneumothorax where surgery is not an option or not ideal for the patient.
Case selection is important; large ruptured bullae, multiple bullas and neoplasia will be much less successful.
How?
Ideally, the patient should have a chest tube(s) in place (to instill blood but also to evacuate air as needed).
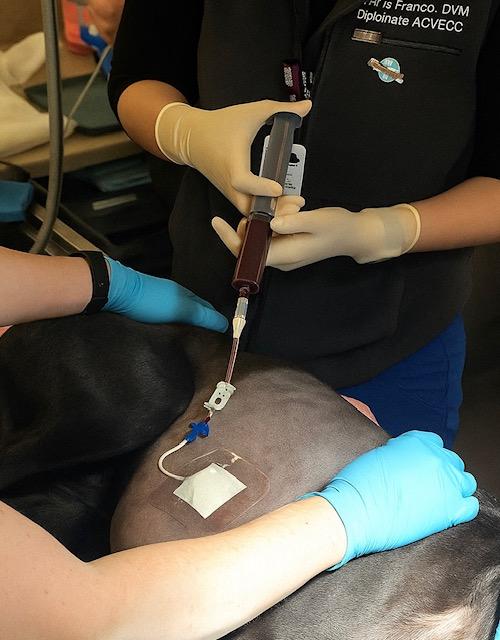
Prep skin over the jugular vein aseptically. Collect approx. 5-10 mL/kg blood using syringe and needle with no additives. A jugular catheter can also be used if appropriate. Collect in 20-35 mL increments until calculated dose achieved.
Inject immediately into pleural cavity via chest tubes. If both sides of the thorax are affected, instill approx. 5 mL/kg into each hemithorax. If only one side is affected, instill 5-10 mL/kg.
Gently rotate the patient to distribute the blood within the thorax.
If chest tubes are in place, flush each tube with 10-20 mL sterile saline.
Do not evacuate the chest tube(s) for at least 4 hours.
Ideally, do not evacuate the chest for the next 24 hours UNLESS the patient is tachypneic/dyspnea.
This procedure is performed aseptically but most clinicians will opt to prescribe a short course of a broad-spectrum antibiotic.
There is a risk of pneumonia/empyema
Efficacy
2021 Case series (5 dogs): 4/5 (80%) resolved after one BPP. The fifth dog lacked immediate response and underwent repeat BPP but died under anesthesia
2014 Case series (8 dogs): 7/8 (87.5%) ultimately succeeded after multiple BPPs, with 62.5% success after a single treatment.
Resources
Oppenheimer, N, et al. Retrospective evaluation of the use of autologous blood-patch treatment for persistent pneumothorax in 8 dogs (2009–2012). JVECC 2014; 24(2): 215-220.
Theron, ML, et al. Autologous blood patch pleurodesis treatment for persistent pneumothorax: A case series of five dogs (2016–2020). Open Vet J, 2021; 11(2): 289-294.